
Types of Treatment
Treatment can be divided into two parts – the treatment of male infertility itself or the treatment as a couple in order to become pregnant.
As research and knowledge stands at the moment, there is currently no treatment for genetically based infertility. Hormonal deficiencies can sometimes be partially corrected with medication, but again this is rare.
Anatomical causes of infertility can sometimes be treated surgically, such as varicoceles. However, there is no direct correlation between surgical correction of varicoceles and increase in fertility, which reflects the controversy of the role of varicoceles in causing male infertility. In some cases, increased levels of prolactin, known as hyperprolactinaemia, can cause oligospermia. Treatment of hyperprolactinaemia with the dopamine agonist bromocriptine can help increase sperm count.
The best course of action is treatment of the couple through various techniques – intrauterine insemination (IUI), in vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI). However, these rely on the production of a semen sample by the man, and therefore may be harder for men experiencing erection or ejaculatory problems.
 Intrauterine insemination (IUI)
Intrauterine insemination (IUI)
IUI is best used for sperm that has mild to moderate abnormalities and still possesses some motility and the ability to penetrate the egg.
IUI is the first treatment step, and is usually done for 3 – 6 months, providing the woman is ovulating properly and the egg can reach the uterus – there is no point doing this procedure if the woman has blocked or damaged fallopian tubes or other problems that would affect egg transport to the site of insemination.
Similar to semen analysis, a semen sample is produced by masturbation, and is washed to produce a smaller, more concentrated sample. The semen is then deposited into the uterus using a catheter.
Image courtesy: https://commons.wikimedia.org/wiki/Image:Penis_Anatomy2.gif (GNU Free Documentation License).
{kind=link}
In vitro fertilisation (IVF)
IVF is the next step for treatment should IUI prove unsuccessful. IVF has a much higher success rate per cycle when compared to IUI, but cannot be used with low sperm count or motility as the sperm still needs to penetrate the egg. The woman’s ovaries must first be stimulated to produce multiple eggs per cycle, which can then be harvested. The eggs are fertilised in a laboratory with her partner’s sperm, and the embryos are allowed to mature for several days. More than one embryo is usually implanted to increase the chance of successful implantation, but can result in twins or triplets. IVF can also be used with donor sperm should the male partner be azoospermic.
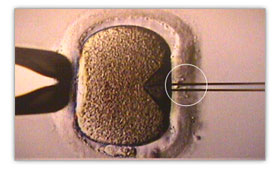
Intracytoplasmic sperm injection (ICSI)
ICSI is very similar to IVF, but instead of co-incubating the sperm and the egg and letting the sperm naturally penetrate and fertilise the egg, ICSI involves the injection of a single sperm straight into the egg. It can be used for severe cases of male infertility, as only one sperm cell is required per egg, and the sperm does not have to be able to swim to or penetrate the egg itself.
Rumour has it that ICSI was developed by accident, when a technician performing IVF slipped and accidentally injected the sperm straight into the egg. He reported his mistake, but found that fertilisation still occurred and produced a viable embryo, providing a more stable technique and a treatment that could also be used for severe male infertility.
In addition to clinical procedures, counselling and psychological evaluations may also prove valuable.
Male infertility may be considered embarrassing, and counselling may help couples come to terms with what is happening and help them be more relaxed and open about treatment.
Many assisted reproduction clinics will put couples in contact with others who are also going seeking treatment for infertility, providing support and information for infertile couples.
Image courtesy: https://commons.wikimedia.org/wiki/Image:Tr_icsi_03.jpg
{kind=link}